
For Researchers
What is Barrett’s esophagus (BE)?
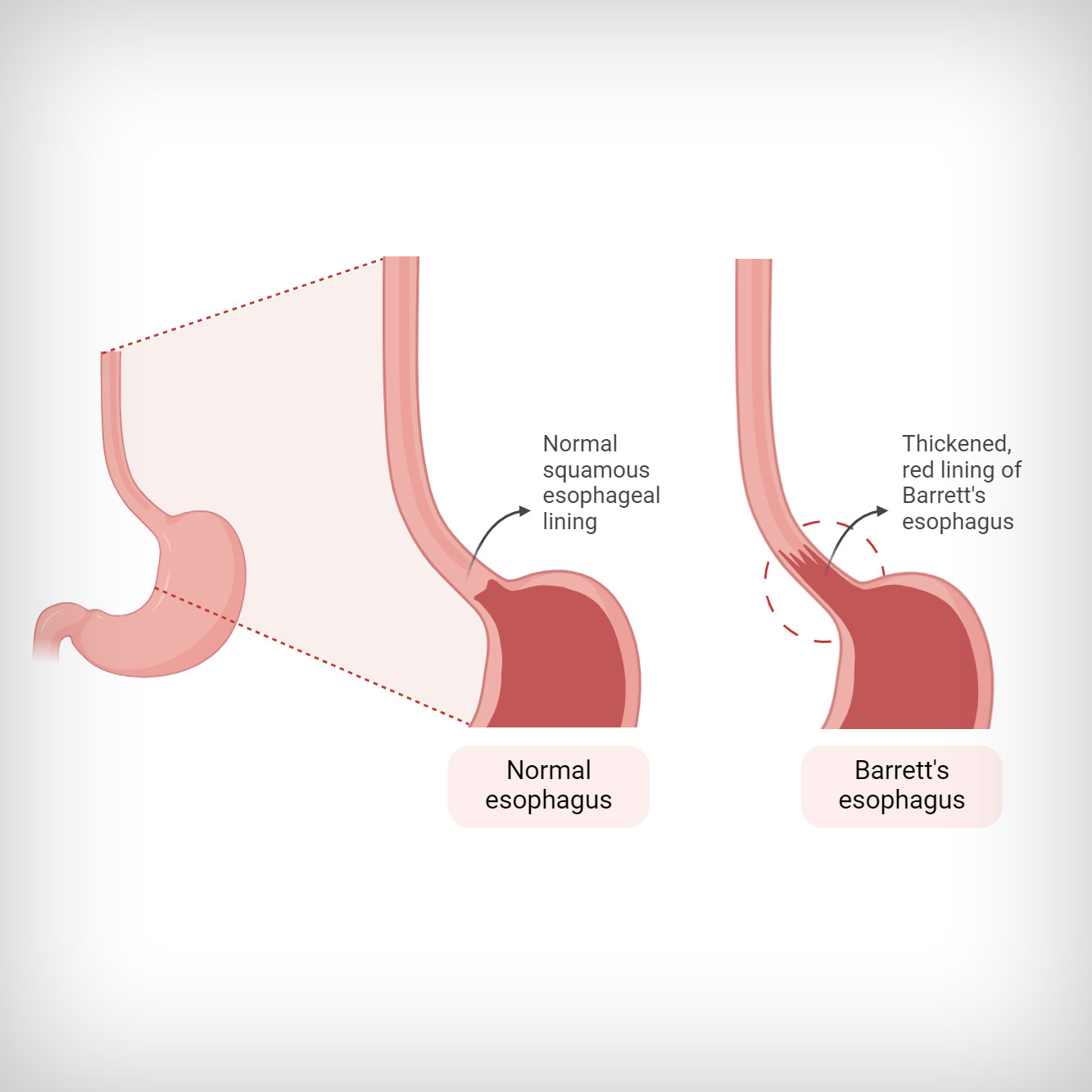
BE is a condition in which the cells that line the lower esophagus are replaced by cells similar to the lining of the intestine. In medical terms, this process is called metaplasia. The exact way of how BE develops is not known; however, it is associated with gastroesophageal reflux disease (GERD). Other risk factors for BE are male gender and Caucasian origin. BE is usually diagnosed around the age of 55.
For Researchers
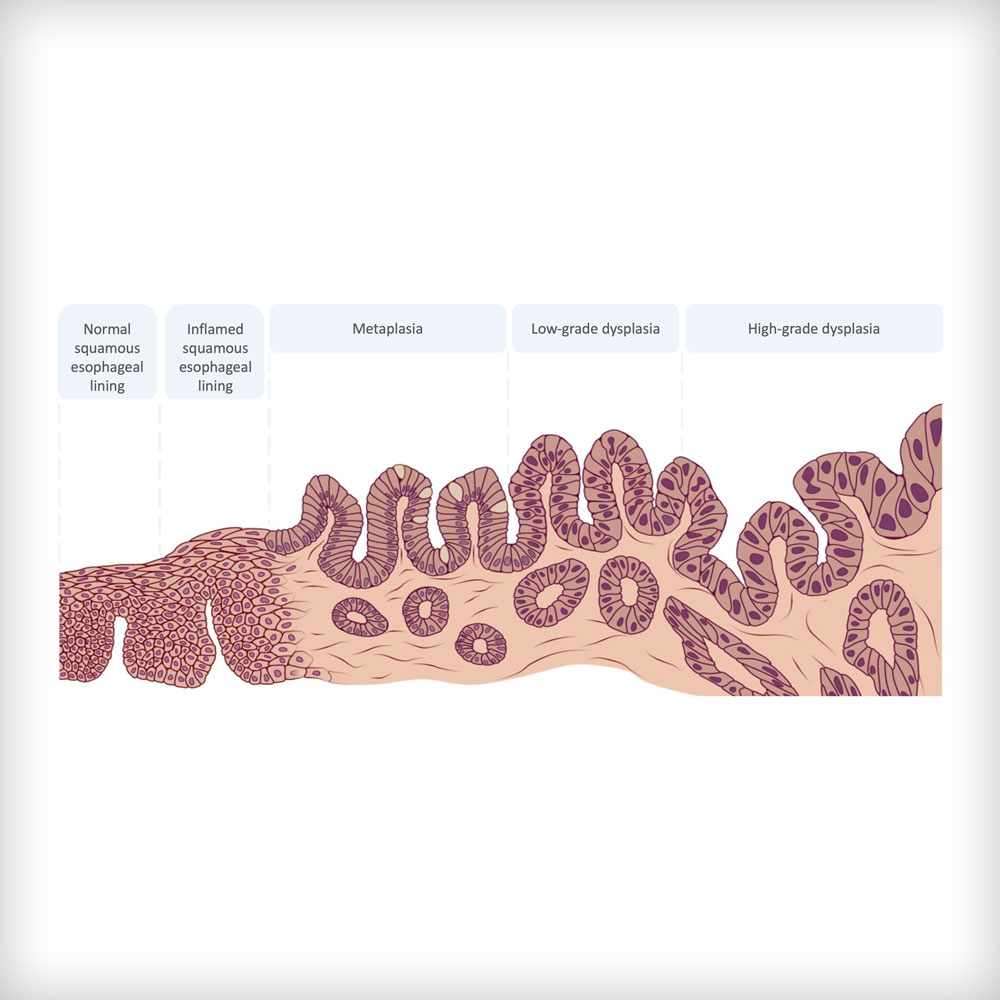
What is the link between Barrett’s esophagus (BE) and esophageal cancer?

For Researchers
Diagnosis of Barrett’s esophagus (BE)?
BE is diagnosed by performing an upper gastrointestinal endoscopy and biopsy. During this endoscopy a trained health care provider, usually a gastroenterologist, looks inside the gastrointestinal tract using an endoscope, a thin tube with a small camera inside. This endoscope is also used to take a small piece of esophageal tissue, a biopsy, which can later be analysed in the laboratory to check for the presence of BE cells. Biopsies are also taken to detect dysplasia. Since dysplasia does not affect all the Barrett tissue, one biopsy is not enough to diagnose dysplasia and multiple biopsy samples, usually from at least four different areas within the Barrett tissue, are taken.
For Researchers
Treatment of Barrett’s esophagus (BE)?
Medication:
Most BE patients suffer from Gastroesophageal Reflux Disease. Acid-suppressing medication will be prescribed to prevent GERD, further esophageal damage, and development of dysplasia and cancer.
Repeated surveillance:
Periodic endoscopies and biopsies to look for cellular changes indicating dysplasia or early cancer. The frequency of surveillance is clearly defined and depends on the status of dysplasia. For example, surveillance will be more frequent in patients with low-grade dysplasia compared to those with no dysplasia.
Endoscopic therapy:
Endoscopic mucosal ablation (EMA):
Ablation is a minimally invasive procedure that will destroy the pre-cancerous cells (dysplasia) in the esophagus. It helps to prevent progression to EAC. No open surgery is needed with this technique.
Endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD):
These techniques are applied to dissect the dysplastic or early cancers from the BE segment. The dysplastic or malignant BE mucosa is cut off and then removed using an endoscope. No open surgery is needed with this technique.
Surgery:
Surgery (esophagectomy) is an alternative to endoscopic therapy or applied in case of more advanced cancer stages. Esophagectomy is a surgical procedure in which almost the entire esophagus is removed. The esophagus is recreated using a part of the stomach or large intestine. Surgery involves more complications. Therefore, endoscopic therapy is preferred if the cancer is still in an early stage.
For Researchers
Visual Overview: Problem, Goal, Impact
Current Problem
Barrett with early cancer
Endoscopic treatment
Stable remission
Recurrent disease
High frequency follow-up for all
- Quality of life for patients
- Healthcare costs
- Patient-centred treatment
Our goal
Use biomarkers to identify Barret patients at high risk
Apply these for risk stratification and directing treatment and follow-up:
- Risk
- Follow-up
- Risk
- Follow-up
Expected impact
- Quality of life for patients
- Healthcare costs
- Patient-centred treatment
For Researchers
Research: Work Packages
- WP1
Project and financial management
- WP2
Design of the study by reaching consensus on standard treatment and using a patient centre approach to define the outcomes of the clinical studies
- Define outcomes
- SOPs
- Final trial design
- WP3
Prospective pilot cohort study for optimising the risk model and correct for gender in preparation of the RCT, and for testing novel HTP methods for assessing clonal diversity for future use
- Ethical approval
- Inclusion of patients
- Sequencing technologies
- WP4
Conduct a prospective our CT4 testing another risk model based surveillance algorithm for patients with early Barrett cancers to assess cost effectiveness, HRQoL and caregivers satisfaction
- Ethical approval
- Performance of the RCT
- Evaluation of the results
- WP5
Health economic modelling and roadmap towards implementation in the healthcare system
- Risk model cost effectiveness
- Sustainability surveillance program evaluation
- Roadmap implementation
- WP6
Communication, dissemination and exploitation
For Researchers